PUERPERAL SEPSIS-GENITAL TRACT INFECTION
GENITAL TRACT INFECTION:
PUERPERAL SEPSIS
INTRODUCTION
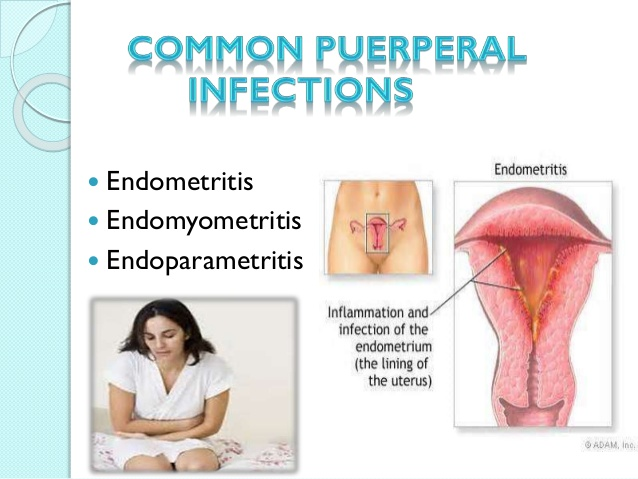
Genital tract infection following delivery is referred to as
Peuperal Sepsis and is synonymous with older descriptions of peuperal fever,
milk fever and child bed fever. It can also be deemed as infection of the
birth canal in the first six weeks following labour or abortion with the
temperature reaching 38 °C or more
for 24 hours, or for at least two days of the first 14 days post delivery due
to entry, growth and multiplication of pathogenic organisms (Sallers, 2010).
Peuperal Sepsis was not realized until the mid 19th
century that the high maternal mortality and morbidity was due to poor hygiene
of birth attendants; the establishment of lying in hospitals and overcrowding
perpetuated the condition to epidemic proportions. Until 1937, peuperal sepsis
was the major cause of maternal mortality. The discovery of the sulphonamides in 1935 and the
simultaneous reduction in the virulence of the hemolytic streptococcus resulted
in a dramatic fall in maternal mortality. As by the year 2000, the incidence of
peuperal sepsis was approximately at 3%.
CAUSES OF PEUPERAL SEPSIS
a) Microorganisms
The causative organisms are either aerobic or anaerobic.
These could be endogenous or exogenous. Endogenous organisms inhabit the bowel,
the anus, the vagina, and the perineum. E. coli is such an example. Exogenous
organisms come from outside of the body. They may be introduced through
procedures from the attendants, in-patients and the environment.
Ø Aerobes
Gram
Positive
-
Beta-haemolytic streptococcus, group A, B and D
-
Staphylococcus epidermis and aureus
-
Enterococci – streptococci
Gram
Positive
-
Escherichia coli
-
Haemophilus influenza
-
Pseudomonous aeruginosa
-
Proteus mirabilis
Gram
variable
-
Gardnerella pneumonea
Ø Anaerobes
-
Peptococcus species
-
Peptostreptococcus sp
-
Bacteroides – B fragilis, B Bivius, B diseus
-
Fusobacterium species
Ø Miscellaneous
-
Mycoplasma hominis
-
Chlamidia trachomatis
-
Mycoplasma urealyticum
b) SOURCES OF
INFECTION
The sources of infection are classified as autogenous,
endogenous and exogenous.
§ Autogenous
sources
The infection is from the patient herself. This may be from
the nose, skin, valve, throat, feaces or any infectious foci.
§ Endogenous
sources
The organisms are readily present in the patient’s vagina.
They may gain entry through tears and bruises in the vagina, cervix and the
uterus.
§ Exogenous
sources
These are from the attendants’ noses, nails, clothes, linen
and the environment. Haemolytic staphylococcus Lance field Group A and
Staphylococci aureus are two exogenous organisms that can cause peuperal
sepsis. The two have been associated with major epidemics and fatalities in the
past.
PREDISPOSING FACTORS
a) OBSTETRIC
FACTORS
v Antenatal
intrauterine infections
v Bruises and
lacerations
v Caesarian
section
v Internal
version
v Cervical
sealage for cervical incompetence
v Prolonged
rapture of membranes
v Untreated
local infections such as Pelvic Inflammatory Diseases
v Multiple
vaginal examinations
v Internal
fetal monitoring
v Instrumental
deliveries
v Prolonged
labour
v Manual
removal of the placenta
v Retained
products of conception
b) NON-OBSTETRIC
FACTORS
v Obesity
v Diabetes
v Anaemia
v HIV
v Mulnutrition
v Exhaustion
(stress)
v Use of
unsterile instruments
v Dirty
environment

SIGNS AND SYMPTOMS
-
Fever which occurs within 24 hours is the first sign
-
Tachycardia
-
Pelvic thrombophlebitis indicated by a persistent
spiking fever for 7 to 10 days after delivery, despite antibiotic therapy
-
Uterus – sub-involuted, boggy, tender and larger
-
Infected wounds – caesarian/perineal
-
Local pain and swelling of the infected suture line
-
Indurated adnaxea (parametritis)
-
Bogginess in the pelvis (absces)
-
Malaise, headache, chills, rigors and insomnia
-
Lower abdominal tenderness and discomfort,
-
Anorexia
-
Diarrheoa
-
Foul smelling lochia (brownish in colour)
-
Secondary post-partum haemorrhage
-
Severe sepsis
Constant pelvic pain
Rise in temperature with increased pulse rate
Lower abdominal pain
Intense pain which worsens the condition of the
patient
Severe infection of the fallopian tubes
Collection of pus in the pouch of douglas

DIAGNOSIS
§ Careful
history and physical examination to exclude the causes of fever
-
General condition during pregenancy
-
Number of vaginal examinations
-
Time of rapture of membranes
-
Place of delivery (Hospital or home delivery)
-
Type of labour and delivery whether prolonged or
instrumental
§ Pelvic ultra-sonogram
(reveals retained products of conception)
§ Laboratory
investigations
-
Mid-stream urine
-
High vaginal swab
-
Blood culture
-
Throat swab full blood count
-
Bleeding and clotting time for disseminated
intravascular coagulation or arterial blood gas
.jpg)

Comments
Post a Comment