Fetal Circulation
FETAL CIRCULATION
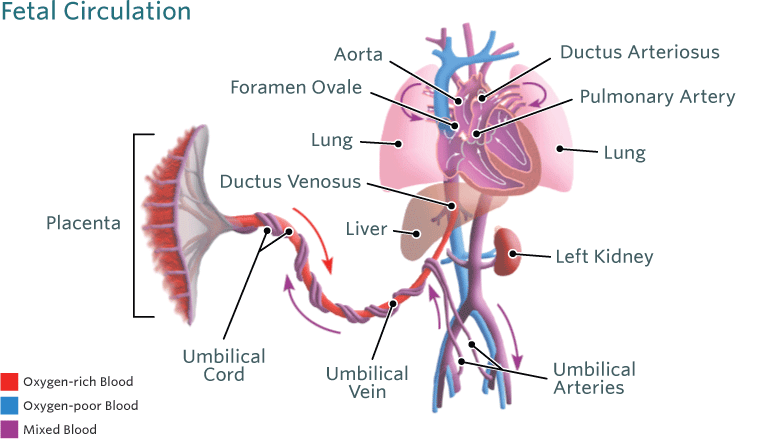
The fetal circulation system is distinctly different from adult circulation. This intricate system allows the fetus to receive oxygenated blood and nutrients from the placenta. It is comprised of the blood vessels in the placenta and the umbilical cord, which contains two umbilical arteries and one umbilical vein. Fetal circulation bypasses the lungs via a shunt known as the ductus arteriosus; the liver is also bypassed via the ductus venosus and blood can travel from the right atrium to the left atrium via the foramen ovale. Normal fetal heart rate is between 110 and 160 peats per minute. When compared to adults, fetuses have decreased ventricular filling and reduced contractility. Fetal circulation undergoes a rapid transition after birth to accommodate extra-uterine life. Human understanding of fetal circulation originated from fetal sheep but ultrasound and magnetic resonance imaging (MRI) during the fetal period now provide detailed information.There are distinct differences in the fetal circulation that if not appropriately formed can lead to childhood or adult diseases.
How does the fetal circulatory system work?
During pregnancy, the fetal circulatory system works differently than after birth:
- The fetus is connected by the umbilical cord to the placenta, the organ that develops and implants in the mother's uterus during pregnancy.
- Through the blood vessels in the umbilical cord, the fetus receives all the necessary nutrition, oxygen, and life support from the mother through the placenta.
- Waste products and carbon dioxide from the fetus are sent back through the umbilical cord and placenta to the mother's circulation to be eliminated.
Comparison to Adults
The adult heart consists of 4 chambers, each with inflow and outflow. Its objective is to take deoxygenated blood from the body, transport it to the lungs for oxygenation, and then take this oxygenated blood to the tissues. For more information on this, you can look at the physiology and anatomy of the heart.
A fetus is surrounded by amniotic fluid and will use the placenta as its source of oxygen and nutrients. While the lungs are developing, they are not functional and provide no oxygenation. There are also high energy demands of developing tissue, in particular the brain. As a result, the fetal circulation must direct blood away from non-functional organs and ensure that growing tissues receive their oxygen requirements.
Fetal Heart structure
Due to these differences, the fetal heart has a number of different structures to direct blood flow:
- The umbilical vein delivers oxygenated blood from the placenta to the fetus, providing oxygen and nutrients.
- The umbilical arteries are used to transport deoxygenated blood away from the fetal tissue and back towards the placenta for re-oxygenation.
- The ductus venosus allows blood from the placenta to bypass the highly demanding, but relatively inactive liver.
- The ductus arteriosus is the fusion of the primitive pulmonary artery to the aorta, therefore allowing blood to pass straight from the right ventricle into the aorta and bypass the inactive lungs.
- The foramen ovale creates a shunt between the right atrium and the left atrium so oxygenated blood from the placenta can move to the left atrium. This allows for the oxygenated blood to pass through the left ventricle and into the ascending aorta, oxygenating the brain.
Oxygen and nutrients from the mother's blood are transferred across the placenta to the fetus. The enriched blood flows through the umbilical cord to the liver and splits into three branches. The blood then reaches the inferior vena cava, a major vein connected to the heart. Most of this blood is sent through the ductus venosus, also a shunt that passes highly oxygenated blood through the liver to the inferior vena cava and then to the right atrium of the heart. A small amount of this blood goes directly to the liver to give it the oxygen and nutrients it needs.
Waste products from the fetal blood are transferred back across the placenta to the mother's blood.
Inside the fetal heart:
Blood enters the right atrium, the chamber on the upper right side of the heart. When the blood enters the right atrium, most of it flows through the foramen ovale into the left atrium.
Blood then passes into the left ventricle (lower chamber of the heart) and then to the aorta, (the large artery coming from the heart).
From the aorta, blood is sent to the heart muscle itself in addition to the brain and arms. After circulating there, the blood returns to the right atrium of the heart through the superior vena cava. Very little of this less oxygenated blood mixes with the oxygenated blood and, instead of going back through the foramen ovale, goes into the right ventricle.
This less oxygenated blood is pumped from the right ventricle into the aorta. A small amount of the blood continues on to the lungs. Most of this blood is shunted through the ductus arteriosus to the descending aorta. This blood then enters the umbilical arteries and flows into the placenta. In the placenta, carbon dioxide and waste products are released into the mother's circulatory system, and oxygen and nutrients from the mother's blood are released into the fetus' blood.
At birth, the umbilical cord is clamped and the baby no longer receives oxygen and nutrients from the mother. With the first breaths of life, the lungs begin to expand. As the lungs expand, the alveoli in the lungs are cleared of fluid. An increase in the baby's blood pressure and a significant reduction in the pulmonary pressures reduces the need for the ductus arteriosus to shunt blood. These changes promote the closure of the shunt. These changes increase the pressure in the left atrium of the heart, which decrease the pressure in the right atrium. The shift in pressure stimulates the foramen ovale to close.
Blood circulation after birth
The closure of the ductus arteriosus and foramen ovale completes the transition of fetal circulation to newborn circulation.
Oxygenation in utero
The highest partial pressure of oxygen in the feto-placental circulation is approximately 4kPa. This is compared to 13kPa in an adult. However, the fetus is able to maintain adequate oxygen delivery to tissues through the use of the shunts above, assisted by a relative polycythaemia and the properties of fetal haemoglobin.
How is fetal haemoglobin different?
Fetal haemoglobin has a different quaternary structure to adult haemoglobin. Adult haemoglobin (HbA) is formed of 2 alpha subunits and 2 beta subunits. However, fetal haemoglobin contains different subunits, namely 2 alpha subunits and 2 gamma subunits.
This change in three dimensional structure of the protein means that fetal haemoglobin can bind more readily to oxygen from maternal circulation. This allows for adequate oxygenation of tissues.
Fetal Heart to Neonatal Heart
The fetal heart undergoes changes during birth to allow the newborn to effectively oxygenate itself with newly open lungs. This occurs in a series of steps:
- The first breath causes a rise in the partial pressure of oxygen
- An increase in partial pressure of oxygen causes pulmonary vasodilation
- Pulmonary vasodilation leads to a drop in right heart pressure.
- Simultaneously, placental circulation ceases, causing left heart pressure to rise.
- These factors combine to cause the foramen ovale to shut.
- The pulmonary and systemic circulations become separate, and the whole output of the right ventricle passes through the pulmonary circulation.
- The final step in the sequence is the closure of the ductus arteriosus, occurring 2 to 3 days after birth.
- The structural remnants of the fetal circulatory structures are referred to as the fossa ovalis (foramen ovale), the ligamentum arteriosum (ductus arteriosus) and the ligamentum venosum (ductus venosus).
.jpg)

Comments
Post a Comment